
“So let me get this straight. At Palisade Direct Primary Care, you don’t charge for visits? And you don’t charge for procedures? How do you even make money?! Will you be okay?”
Oftentimes when I explain how much value Direct Primary Care brings to a patient, I’m met with a blank stare. Sometimes incredulity. How is it even possible for this model to be financially sustainable?
It’s simpler than you’d think.
First, story time!
The Administrator Apocalypse
Once upon a time, there were two people. The first had a medical degree. The second had a medical problem. The first helped the second, and the second paid the first. It was a simple time. It was a good time.
And then this happened:
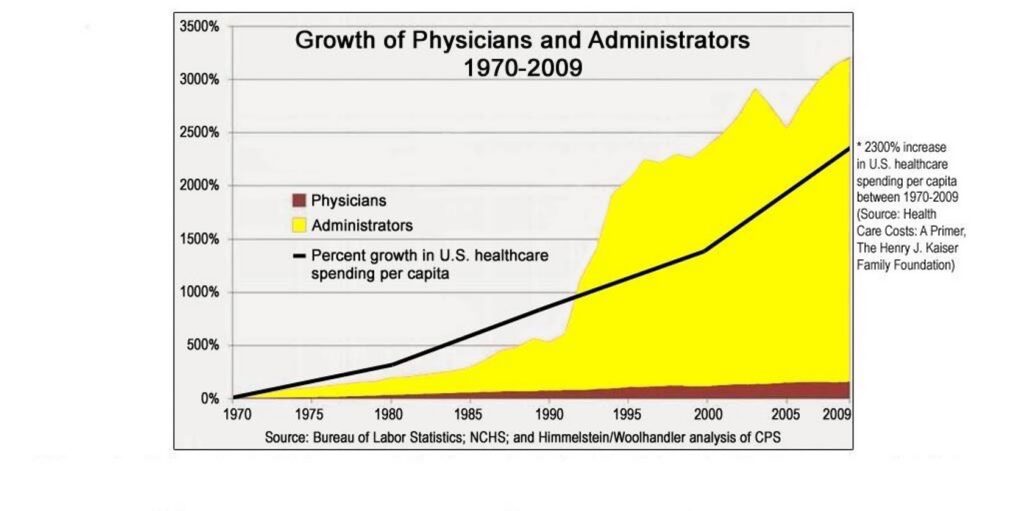
Now, there are many legitimate reasons for such an increase in healthcare administration. Medications and procedures became more complex and needed management. Medicare/Medicaid regulations focused on improving health outcomes for American citizens, and healthcare systems needed to hire people to figure out how to best address those regulations.
But somewhere along the way, insurance companies hired administrators to find creative ways to save money. Then those administrators needed supervising administrators. Then the healthcare system needed to hire administrators to address the demands from the administrators on the payor side. And those administrators needed managing administrators.
Rinse, repeat, the above chart was born.
Pass The Buck
Instead of building a system of healthcare around the patient, it very quickly became a system of healthcare for the System’s sake. The heart of medicine was lost.
Health decisions between a physician and their patient became insurance company driven requirements.
The warmth of an in-person visit became a generic mass email.
Your doctor’s receptionist became a call center – or worse – a kiosk.
Along with all of this administrative complexity came exponential cost increases, which ultimately passed on to the patient.
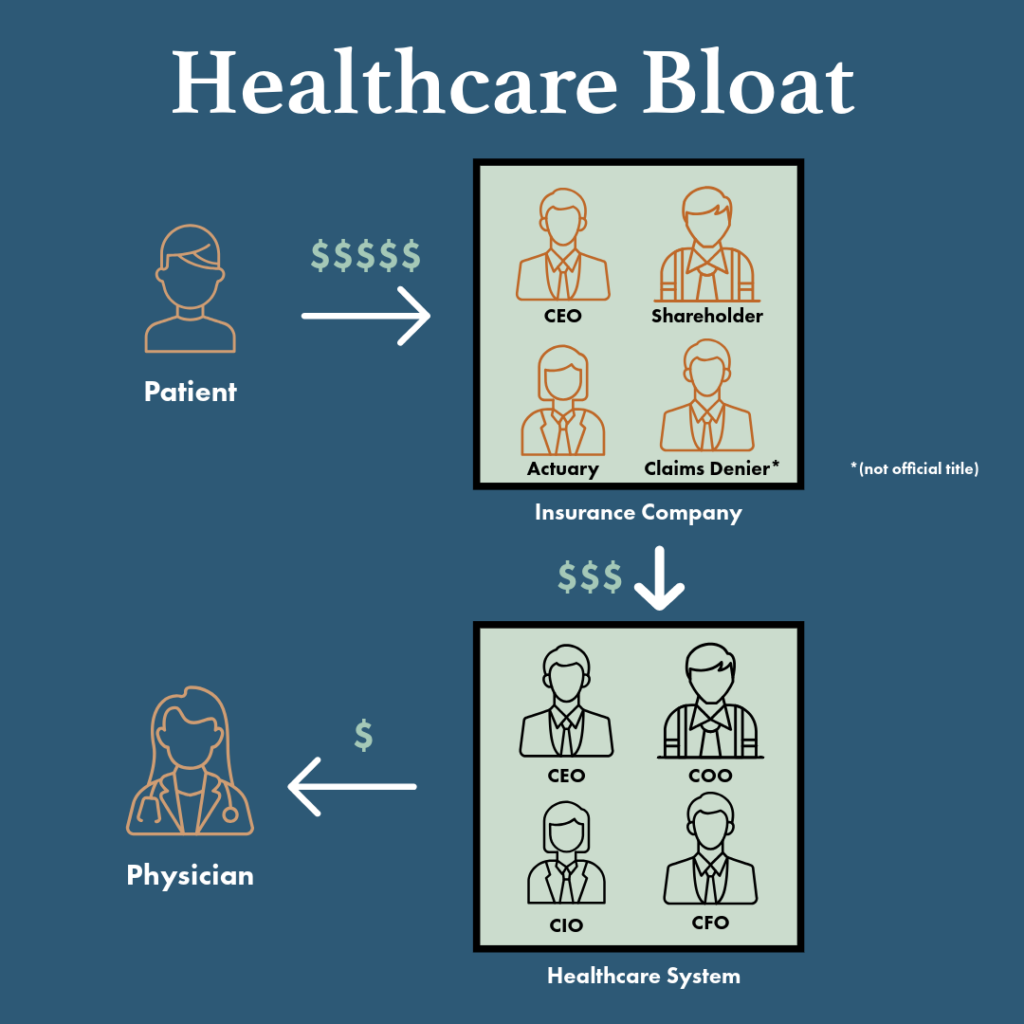
Standard 20-minute office visits became $450. Your child has an ear infection and it happens to be their well child visit? $450. You have your annual physical and you need medications refilled? $450. Oh, you need labs as well? Those labs (with the lab draw fee) are $500-$1000.
Not only does administrative bloat increase cost to the patient, but it also hurts your physician. Did you know that your family physician is expected to have 2000-3000 patients on their panel?
That means that there are 2000-3000 other people that call your doctor, “My doctor.” This is considered “sustainable” for an insurance-reimbursed practice. You need to pay for all of those layers of complexity somehow. A physician that sees 10 patients a day is not “sustainable” for the practice, but a physician who sees 30 patients a day? Now we’re cooking.
Speaking as someone who lived in that system, it is exhausting. It’s why so many physicians are burning out and leaving healthcare altogether.
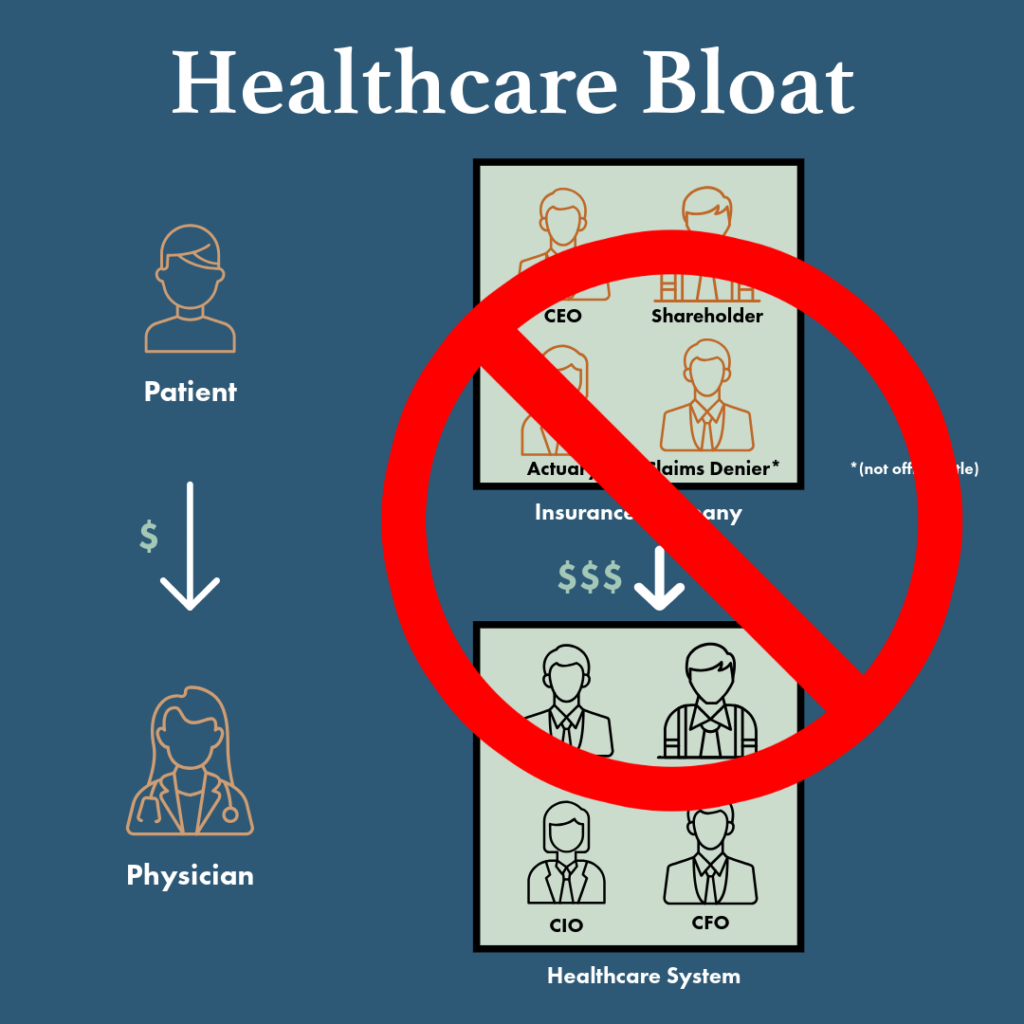
The Direct Primary Care Difference
Meanwhile, all across the country, doctors found ways to break the mold. Pay $50-$100 per month, and you get unlimited visits with no extra copay. Avoid insurance altogether, and your labs are <5% the cost of the big healthcare system.
You get to call your doctor and actually talk to them. Same-day or next-day appointments are no longer shunted to urgent care.
Your visits are not rushed because your doctor is no longer incentivized to see as many patients in a day as possible. Their incentive is to keep you healthy, happy, and living your best life.
With Direct Primary Care, the only people involved in your health are you and your physician. Under this model, the “sustainable” patient panel is around 500 patients, which means 4-5x more time with your doctor.
The old-school family doctor doing home visits for the sick and frail is now possible again.
How Can Direct Primary Care Exist?
There’s no middle men. That’s it.
It’s more cost effective.
It’s more patient-centered.
It’s more sustainable for physicians.
I genuinely believe it is the future of healthcare.